



Somebody just said the words "autism spectrum disorder" about your child, and now you're here, reading this on your phone at an hour you'd normally be asleep. That's an extremely normal way to end up on this page.
Here's the short version. Autism is a difference in how a brain develops and takes in the world. It isn't an illness. It isn't caused by anything you did. And it isn't a preview of a hard life. It does mean your child's brain handles communication, connection, and sensory input differently than most brains do. What that looks like day to day varies enormously from one child to the next, which is the entire reason the word "spectrum" exists in the first place.
Forget the Mild-to-Severe Line
Most people picture the spectrum as a ruler: mild at one end, severe at the other, your child parked somewhere along it. That picture is wrong, and it wastes a lot of parental energy on the wrong question — figuring out where a kid "ranks" instead of what they need this week.
A better model is a soundboard with a dozen independent dials, or a color wheel where every color can be turned up or down on its own. One dial might sit high — say an advanced vocabulary or a scary-good memory for dinosaur names — while a completely unrelated dial sits low, like a full meltdown at the sound of a hand dryer. Neither dial cancels out the other. They both just exist, at the same time, in the same kid.
Two children can carry the exact same diagnosis and look almost nothing alike. That's not a contradiction in the diagnosis. That is the diagnosis.
What It Tends to Look Like
Social communication is usually the first thing parents notice, even before they have a name for it. Instead of pointing at a toy and glancing back at you to share the moment (what specialists call joint attention), a toddler might just grab your wrist and walk you to the shelf — no eye contact required. Years later, that same wiring can show up as an eight-year-old delivering a detailed, unbroken briefing on pteranodon wingspan long after the listener has mentally checked out. Neither behavior is rudeness. It's a different set of instincts about what counts as a shared moment.
Repetitive behavior and routine covers a wide range: lining up toy cars in a precise order, and real distress when someone "helpfully" fixes the line; rocking, hand-flapping, or humming when a feeling gets too big to sit still through. That last category — usually called stimming — isn't a symptom to eliminate. It's typically the nervous system's own way of regulating itself, and removing it without offering something else that actually works tends to make things harder, not easier.
Sensory processing differences run in both directions. Some kids are hyper-reactive: a vacuum cleaner is physically painful, clothing tags feel like sandpaper, fluorescent lights are unbearable. Others are hypo-reactive and seem to seek input — crashing into couch cushions, craving tight bear hugs, chewing on shirt collars. A lot of behavior that gets labeled as defiance is a sensory system asking loudly for something it has no quieter way to ask for.
What the Research Says Right Now
The science here has moved fast over the past year, and some of it is genuinely worth knowing.
Autism identification has climbed for two decades straight. The CDC's most recent surveillance data, released in 2025, put the number at about 1 in 31 eight-year-olds in the U.S., up from 1 in 150 in 2000.
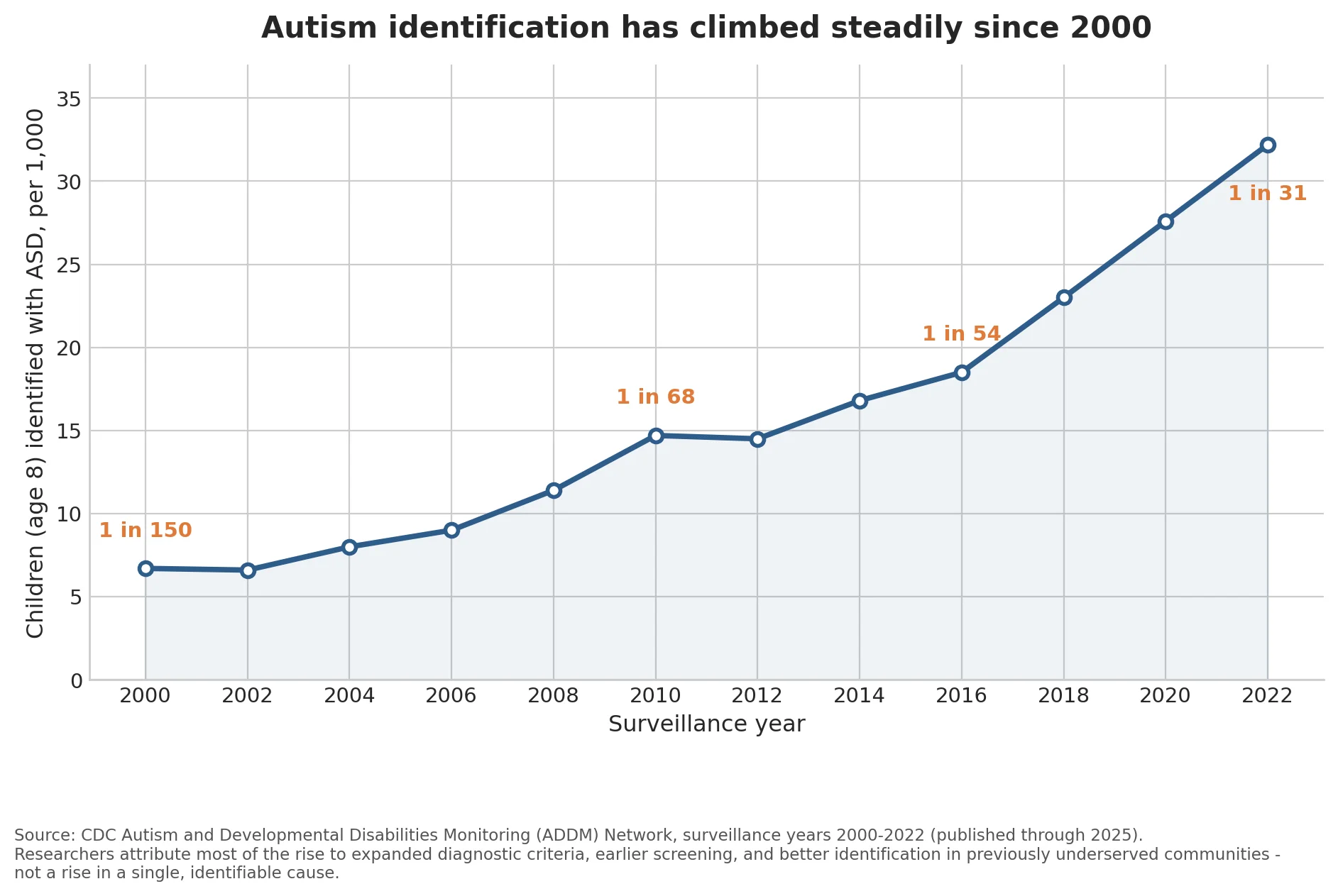
That's a real number, but it isn't evidence of a sudden outbreak. Researchers who run the surveillance point to a mix of causes: wider diagnostic criteria, screening that starts earlier, and — probably the biggest factor — far better identification in communities that used to be overlooked entirely. A rising line on this chart mostly means more kids are being seen. It doesn't mean more kids are suddenly different.
Autism also isn't one thing biologically, and there's now data behind that. In July 2025, researchers at Princeton University and the Simons Foundation published a study in Nature Genetics that sorted more than 5,000 autistic children into groups based on over 230 individual traits, then checked whether those groups lined up with distinct genetics. They did, cleanly enough that the team could replicate the same four groups in a second, separate sample. Researchers named the four profiles: Social and Behavioral Challenges, Mixed ASD with Developmental Delay, Moderate Challenges, and Broadly Affected. None of them map onto the old idea of "high-functioning" versus "low-functioning." They map onto different underlying biology entirely — which is exactly why a one-size-fits-all approach to support was never going to work well.
And the overlap with ADHD keeps getting harder to ignore. Genetic studies have linked shared risk variants between the two conditions for years. A 2025 brain-imaging study from the Child Mind Institute added something more specific: in children diagnosed with either autism or ADHD, the strength of autism-related traits — not which diagnosis was written on the chart — predicted the same pattern of brain connectivity and the same genes switching on. The brain, it turns out, doesn't sort itself neatly into the two labels used in the clinic. A lot of children living with both sets of traits (sometimes called AuDHD) are dealing with one underlying picture wearing two different diagnostic hats.
What Actually Helps at Home
None of this changes who your child is. It changes what's worth spending your energy on.
Functional communication comes before everything else on this list. However your child communicates — spoken words, sign, a picture exchange system, an AAC device — the immediate goal is giving them a reliable way to say "I need a break" or "that's too loud" or "I want water." A child who can get a basic need across has a lot less reason to melt down trying to get it across some other way.
Their interests aren't a distraction from learning. They're the fastest route into it. A kid obsessed with trains can learn counting, reading, and turn-taking through trains specifically, faster than through worksheets about something they don't care about. Following the interest isn't spoiling the child. It's using motivation that already exists instead of manufacturing a fake one.
Predictability does a lot of quiet work. A visual schedule, or a plain warning before a transition ("five more minutes, then we're leaving"), removes a huge amount of the uncertainty that makes an ordinary day feel unsafe. It costs you almost nothing and tends to pay off immediately.
One more thing worth saying plainly: you don't need to extinguish every stim, force eye contact, or chase "indistinguishable from peers" as a goal. Those used to be standard therapy targets. A lot of autistic adults who grew up under that model have since said, clearly and often, that being trained out of their own regulation strategies cost them more than it ever helped. The goal that's aged better is a child who can function, communicate, and feel safe in their own skin — not a child who looks like everyone else.
You don't have to have all of this figured out tonight. Understanding your child's specific profile — which dials sit high and which sit low — is a process that unfolds over years, usually with input from a pediatrician, a developmental specialist, or both. For now, it's enough to know that the diagnosis you just heard describes a different way of experiencing the world. Not a smaller one.
This article is for general understanding and isn't a substitute for an evaluation from a pediatrician, developmental pediatrician, or psychologist. If you have concerns about your child's development, they're worth raising with one directly.
Sources: CDC Autism and Developmental Disabilities Monitoring (ADDM) Network, 2025 surveillance report; Litman, Sauerwald, et al., Nature Genetics, July 2025 (Princeton University / Simons Foundation); Di Martino et al., Molecular Psychiatry, 2025 (Child Mind Institute).
